- Caffeine International Labor Organization
- Cafcit® (caffeine citrate) injection and oral solution U.S. Food and Drug Administration
- Mattia A, 2013, Regulatory status of caffeine National Institute of Health, Office of Dietary Supplements
- Caffeine U.S. Food and Drug Administration
- Initial processing Coffee and Health
- Isolation of caffeine from tea New Mexico Institute of Mining and Technology
- Kola nut plant Encyclopaedia Britannica
- Does cocoa contain caffeine? Food-Info
- Caffeine Encyclopedia of Life
- Caffeine content for coffee, tea, soda and more Mayo Clinic
- Caffeine content of drinks Caffeine Informer
- Foods highest in caffeine NutritionData
- Energy Drinks Brown University
- Assurance of voluntary compliance and voluntary discontinuance State of California – Department of Justice
- How much caffeine is in tea? Choice Organic Teas
- Neurologic effects of caffeine Emedicine
- Attwood AS et al, Caffeinated alcohol beverages: a public health concern PubMed
- Caffeine and alcohol Centers of Disease Control and Prevention
- Heaney RP, 2002, Effects of caffeine on bone and the calcium economy PubMed
- Caffeine pregnancy and breastfeeding warnings Drugs.com
- 2010, Moderate Caffeine Consumption During Pregnancy The American Congress of Obstetricians and Gynecologists
- Coffee Linus Pauling Institute
- Pimentel GD et al, 2009, Does long-term coffee intake reduce type 2 diabetes mellitus risk? PubMed
- Caffeine Drugs.com
- Fredholm BB et al, 1999, Actions of Caffeine in the Brain with Special Reference to Factors That Contribute to Its Widespread Use Pharmacological Reviews
- Aranda JV et al, 1979, Maturation of caffeine elimination in infancy Archives of Disease in Childhood
- Yew D, Caffeine toxicity Emedicine
- de Wijkersloth LRH et al, Life-threatening hypokalaemia and lactate accumulation after autointoxication with Stacker 2®, a ‘powerful slimming agent PubMed Central
- Pharmacology of caffeine The National Academic Press
- Caffeine (anhydrous) Sigma-Aldrich
- Keijzers GB et al, 2002, Caffeine Can Decrease Insulin Sensitivity in Humans Diabetes Care
- Robertson D et al, 1981, Tolerance to the Humoral and Hemodynamic Effects of Caffeine in Man PubMed Central
- Norager CB et al, 2006, Metabolic effects of caffeine ingestion and physical work in 75-year old citizens. A randomized, double-blind, placebo-controlled, cross-over study PubMed
- Caffeine in food Caffeine Informer
- Caffeine in workout supplements Caffeine Informer
- Dekker MJ et al, 2007, Glucose homeostasis remains altered by acute caffeine ingestion following 2 weeks of daily caffeine consumption in previously non-caffeine-consuming males PubMed
- Gavrieli A et al, 2011, Caffeinated Coffee Does Not Acutely Affect Energy Intake, Appetite, or Inflammation but Prevents Serum Cortisol Concentrations from Falling in Healthy Men The Journal of Nutrition
- Mora-Rodríguez R et al, Caffeine Ingestion Reverses the Circadian Rhythm Effects on Neuromuscular Performance in Highly Resistance-Trained Men PubMed
- Lovallo RL et al, 2005, Caffeine Stimulation of Cortisol Secretion Across the Waking Hours in Relation to Caffeine Intake Levels PubMed Central
- Acheson KJ et al, 1980, Caffeine and coffee: their influence on metabolic rate and substrate utilization in normal weight and obese individuals The American Journal of Clinical Nutrition
- Yoshida T et al, 1994, Relationship between basal metabolic rate, thermogenic response to caffeine, and body weight loss following combined low calorie and exercise treatment in obese women PubMed
- Acheson KJ et al, 2004, Metabolic effects of caffeine in humans: lipid oxidation or futile cycling? The American Journal of Clinical Nutrition
- Zahorska-Markiewicz B, 1980, The thermic effect of caffeinated and decaffeinated coffee ingested with breakfast PubMed
- Duloo AG et al, 1989, Normal caffeine consumption: influence on thermogenesis and daily energy expenditure in lean and postobese human volunteers The American Journal of Clinical Nutrition
- Del Coso J et al, 2012, Dose response effects of a caffeine-containing energy drink on muscle performance: a repeated measures design Journal of The International Society of Sport Nutrition
- Hoffman JR et al, 2006, Thermogenic Effect from Nutritionally Enriched Coffee Consumption PubMed Central
- Drake C et al, 2013, Caffeine Effects on Sleep Taken 0, 3, or 6 Hours before Going to Bed Journal of Clinical Sleep Medicine
- Caffeine: How much is too much? Mayo Clinic
- 2012, Regular, moderate, coffee drinking may reduce heart failure risk Heart.org
- Landolt HP, 2012, “No Thanks, Coffee Keeps Me Awake”: Individual Caffeine Sensitivity Depends on ADORA2A Genotype PubMed Central
- Reissig CJ et al, 2009, Caffeinated Energy Drinks — A Growing Problem PubMed Central
- Kim TW et al, 2011, Caffeine increases sweating sensitivity via changes in sudomotor activity during physical loading PubMed
- Jessen AB et al, 2003, Effect of chewing gum containing nicotine and caffeine on energy expenditure and substrate utilization in men The American Journal of Clinical Nutrition
- Belza A et al, 2009, The effect of caffeine, green tea and tyrosine on thermogenesis and energy intake PubMed
- Lotshaw SC et al, 1996, Illustrating caffeine’s pharmacological and expectancy effects utilizing a balanced placebo design PubMed
- Filmore M et al, 1992, Expected effect of caffeine on motor performance predicts the type of response to placebo
PubMed - Snel J et al, 2011, Effects of caffeine on sleep and cognition PubMed
- Brice C et al, 2001, The effects of caffeine on simulated driving, subjective alertness and sustained attention PubMed
- Wesensten NJ et al, 2005, Performance and alertness effects of caffeine, dextroamphetamine, and modafinil during sleep deprivation PubMed
- Winston AP et al, 2005, Neuropsychiatric effects of caffeine BJPsych Advances
- Penetar D et al, 1993, Caffeine reversal of sleep deprivation effects on alertness and mood PubMed
- Ker K et al, 2010, Caffeine for the prevention of injuries and errors in shift workers PubMed
- Mesas AE et al, 2011, The effect of coffee on blood pressure and cardiovascular disease in hypertensive individuals: a systematic review and meta-analysis PubMed
- Spradley BD et al, 2012, Ingesting a pre-workout supplement containing caffeine, B-vitamins, amino acids, creatine, and beta-alanine before exercise delays fatigue while improving reaction time and muscular endurance Nutrition and Metabolism
- Addicott MA at al, 2009, A comparison of the effects of caffeine following abstinence and normal caffeine use PubMed
- James JE et al, 2005, Effects of caffeine on performance and mood: withdrawal reversal is the most plausible explanation PubMed
- Nehlig A, 2010, Is caffeine a cognitive enhancer? PubMed
- Jones G et al, 2008, Caffeine and other sympathomimetic stimulants: modes of action and effects on sports performance PubMed
- Zhang Y et al, 2015, Caffeine and diuresis during rest and exercise: A meta-analysis PubMed
- Ding M et al, 2014, Long-Term Coffee Consumption and Risk of Cardiovascular Disease: A Systematic Review and a Dose-Response Meta-Analysis of Prospective Cohort Studies PubMed
- Robertson D et al, 1978, Effects of caffeine on plasma renin activity, catecholamines and blood pressure PubMed
- Derry CJ et al, 2012, Caffeine as an analgesic adjuvant for acute pain in adults PubMed
- Renner B et al, Caffeine accelerates absorption and enhances the analgesic effect of acetaminophen PubMed
- Diamond S et al, 2000, Ibuprofen plus caffeine in the treatment of tension-type headache PubMed
- Migliardi JR et al, 1994, Caffeine as an analgesic adjuvant in tension headache PubMed
- Greenberg JA et al, 2007, Caffeinated beverage intake and the risk of heart disease mortality in the elderly: a prospective analysis The American Journal of Clinical Nutrition
- Heseltine D et al, 1991, The effect of caffeine on postprandial hypotension in the elderly, PubMed
- Caffeine RxList.com
- Understanding Prostate Changes: A Health Guide for Men National Cancer Institute
- Ziemssen T et al, 2010, Treatment of dysautonomia in extrapyramidal disorders PubMed Central
- Dworetzky DA et al, 2010, A prospective study of smoking, caffeine, and alcohol as risk factors for seizures or epilepsy in young adult women: Data from the Nurses’ Health Study II PubMed Central
- Chroœciñska-Krawczyk M et al, 2011, Caffeine and the anticonvulsant potency of antiepileptic drugs: experimental and clinical data Institute of Pharmacology, Polish Academy of Sciences
- Choi HK et al, 2007, Coffee consumption and risk of incident gout in men: a prospective study PubMed
- Choi HK et al, 2010, Coffee consumption and risk of incident gout in women: the Nurses’ Health Study PubMed
- Welsh EJ et al, 2010, The effect of caffeine in people with asthma Cochrane
- Yurach MT et al, 2011, The effect of caffeinated coffee on airway response to methacholine and exhaled nitric oxide PubMed
- Ishizuk Z et al, 2003, Relation of coffee, green tea, and caffeine intake to gallstone disease in middle-aged Japanese men PubMed
- Walcher T et al, 2010, The effect of alcohol, tobacco and caffeine consumption and vegetarian diet on gallstone prevalence PubMed
- Lara DR, 2010, Caffeine, mental health, and psychiatric disorders PubMed
- Berkey CS et al, 2008, Weight gain in older adolescent females: the internet, sleep, coffee, and alcohol PubMed
- Armstrong LE et al, 2007, Caffeine, Fluid-Electrolyte Balance, Temperature Regulation, and Exercise-Heat Tolerance Medscape
- Maughan RJ et al, 2003, Caffeine ingestion and fluid balance: a review PubMed
- Armstrong LE et al, 2007, Caffeine, Fluid-Electrolyte Balance, Temperature Regulation, and Exercise-Heat Tolerance Medscape
- Lopez-Garcia E et al, 2009, Coffee consumption and risk of stroke in women PubMed
- Zhang J et al, 1998, Inhibition of salivary amylase by black and green teas and their effects on the intraoral hydrolysis of starch PubMed
- Caffeine and your child KidsHealth
- Broderick P et al, 2004, Caffeine and psychiatric symptoms: a review PubMed
- Premenstrual dysphoric disorder MedlinePlus
- Dickerson LM et al, 2003, Premenstrual syndrome American Family Physician
- Caffeine (oral route, parenteral route) Drugs.com
- Boekema PJ et al, 1999, Coffee and gastrointestinal function: facts and fiction. A review PubMed
- Schwartz MD et al, 2002, Dyspepsia, peptic ulcer disease, and esophageal reflux disease PubMed Central
- Efficacy of caffeine The National Academic Press
- Belza A et al, 2009, The effect of caffeine, green tea and tyrosine on thermogenesis and energy intake PubMed
- Caffeine side effects Drugs.com
- Kerrigan S et al, 2009, Fatal caffeine overdose: two case reports PubMed Central
- Yew D, Caffeine Toxicity Clinical Presentation Emedicine
- Caffeine TOXNET
- Tayima Y, 2010, Coffee-induced Hypokalaemia PubMed Central
- Appel CC et al, 2001, Caffeine-induced hypokalemic paralysis in pregnancy PubMed
- Jaslow R, April 20, 2012, Drinking gallons of Coca-Cola daily cited in 30-year-old New Zealand mom’s death CBS News
- Mudge DW et al, 2004, Coca-Cola and kangaroos Gasdoc.de
- 2010, Notice of GRAS Exemption Claim for Use of Caffeine in Alcoholic Beverages U.S. Food and Drug Administration
- Rudolph T et al, 2010, A case of fatal caffeine poisoning PubMed
- Caffeine uses and effectiveness WebMD
- Hartley TR et al, 2000, Hypertension Risk Status and Effect of Caffeine on Blood Pressure Hypertension
- Zhang Z et al, 2011, Habitual coffee consumption and risk of hypertension: a systematic review and meta-analysis of prospective observational studies The American Journal of Clinical Nutrition
- Stafstrom CE, 2004, Dietary Approaches to Epilepsy Treatment: Old and New Options on the Menu PubMed Central
- Restless leg syndrome fact sheet National Institute of Neurological Disorders and Stroke
- Cotter PE et al, 2006, Restless leg syndrome: is it a real problem? PubMed Central
- Hedges DW et al, 2009, Caffeine-induced psychosis PubMed
- Bullough B et al, 1990, Methylxanthines and fibrocystic breast disease: a study of correlations PubMed
- Hallström H et al, 2006, Coffee, tea and caffeine consumption in relation to osteoporotic fracture risk in a cohort of Swedish women PubMed
- Evans SM et al, 1992, Caffeine tolerance and choice in humans PubMed
- Griffiths RR et al, 2000, Caffeine: A drug of abuse? American College of Neuropsychopharmacology
- Farag NH et al, 2005, Caffeine Tolerance is Incomplete: Persistent Blood Pressure Responses in the Ambulatory Setting PubMed Central
- Watson J et al, 2002, Central and peripheral effects of sustained caffeine use: tolerance is incomplete PubMed Central
- Rogers PJ et al, Regular caffeine consumption: a balance of adverse and beneficial effects for mood and psychomotor performance PubMed
- James JE et al, 2005, Dietary caffeine, performance and mood: enhancing and restorative effects after controlling for withdrawal reversal PubMed
- Dews PB et al, The frequency of caffeine withdrawal in a population-based survey and in a controlled, blinded pilot experiment PubMed
- Phillips-Bute BG et al, 1997, Caffeine withdrawal symptoms following brief caffeine deprivation PubMed
- Juliano LM et al, 2004, A critical review of caffeine withdrawal: empirical validation of symptoms and signs, incidence, severity, and associated features Springer Link
- Waugh EJ et al, 2009, Risk factors for low bone mass in healthy 40-60 year old women: a systematic review of the literature PubMed
- Gershon P et al, 2009, Evaluation of experience-based fatigue countermeasures PubMed
- Reyner LA et al, Efficacy of a ‘functional energy drink’ in counteracting driver sleepiness PubMed
- Steffen M et al, 2012, The effect of coffee consumption on blood pressure and the development of hypertension: a systematic review and meta-analysis
PubMed - S6. Stimulants World Anti-Doping Agency
- Astorino TA, 2010, Efficacy of acute caffeine ingestion for short-term high-intensity exercise performance: a systematic review PubMed
- Nehlig A et al, 1994, Caffeine and sports activity: a review PubMed
- Ivy JL et al, 2009, Improved cycling time-trial performance after ingestion of a caffeine energy drink PubMed
- Armstrong LE et al, 2005, Fluid, electrolyte, and renal indices of hydration during 11 days of controlled caffeine consumption PubMed
- Gwacham N et al, 2012, Acute effects of a caffeine-taurine energy drink on repeated sprint performance of American college football players PubMed
- Williams AD et al, 2008, The effect of ephedra and caffeine on maximal strength and power in resistance-trained athletes PubMed
- Crowe MJ et al, Physiological and cognitive responses to caffeine during repeated, high-intensity exercise PubMed
- Carr A et al, 2008, Effect of caffeine supplementation on repeated sprint running performance PubMed
- Paton CD et al, 2010, Caffeinated chewing gum increases repeated sprint performance and augments increases in testosterone in competitive cyclists PubMed
- Collomp K et al, 1992, Benefits of caffeine ingestion on sprint performance in trained and untrained swimmers PubMed
- Coso JD et al, 2012, Effects of a Caffeine-Containing Energy Drink on Simulated Soccer Performance PubMed Central
- Gant N et al, 2010, The influence of caffeine and carbohydrate coingestion on simulated soccer performance PubMed
- Henderson-Smart et al, 2001, Prophylactic caffeine to prevent postoperative apnoea following general anaesthesia in preterm infants Cochrane
- Pedersen DJ et al, 2008, High rates of muscle glycogen resynthesis after exhaustive exercise when carbohydrate is coingested with caffeine PubMed
- McClaran SR et al, 2007, Low doses of caffeine reduce heart rate during submaximal cycle ergometry PubMed
- Van Nieuwenhoven MA et al, 2000, Gastrointestinal function during exercise: comparison of water, sports drink, and sports drink with caffeine Journal of Applied Physiology
- Graham TE et al, Metabolic, catecholamine, and exercise performance responses to various doses of caffeine PubMed
- Davis JK et al, 2009, Caffeine and anaerobic performance: ergogenic value and mechanisms of action PubMed
- Battram DS et al, 2007, The effect of caffeine on glucose kinetics in humans – influence of adrenaline PubMed
- Yeo SE et al, 2005, Caffeine increases exogenous carbohydrate oxidation during exercise PubMed
- Whitehead N et al, 2013, Systematic review of randomised controlled trials of the effects of caffeine or caffeinated drinks on blood glucose concentrations and insulin sensitivity in people with diabetes mellitus PubMed
- Muramakami K et al, 2005, Effect of dietary factors on incidence of type 2 diabetes: a systematic review of cohort studies PubMed
- Van Dongen HP et al, 2001, Caffeine eliminates psychomotor vigilance deficits from sleep inertia PubMed
- Mednick SC et al, 2008, Comparing the benefits of Caffeine, Naps and Placebo on Verbal, Motor and Perceptual Memory PubMed Central
- Hursel R et al, 2009, Green tea catechin plus caffeine supplementation to a high-protein diet has no additional effect on body weight maintenance after weight loss PubMed
- Westerterp-Plantenga MS, 2005, Body weight loss and weight maintenance in relation to habitual caffeine intake and green tea supplementation PubMed
- Tremblay A et al, 1988, Caffeine reduces spontaneous energy intake in men but not in women ScienceDirect
- Astrup A et al, 1992, The effect and safety of an ephedrine/caffeine compound compared to ephedrine, caffeine and placebo in obese subjects on an energy restricted diet. A double blind trial PubMed
- Hackman RM et al, 2006, Multinutrient supplement containing ephedra and caffeine causes weight loss and improves metabolic risk factors in obese women: a randomized controlled trial PubMed
- 2004, Ephedra and Ephedrine Alkaloids for Weight Loss and Athletic Performance National Institute of Health, Office of Dietary Supplements
- Astrup A et al, 1992, The effect and safety of an ephedrine/caffeine compound compared to ephedrine, caffeine and placebo in obese subjects on an energy restricted diet. A double blind trial PubMed
- Black Tea MedlinePlus
- Green Tea WebMD
- Ward N et al, 1991, The analgesic effects of caffeine in headache PubMed
- Haag G et al, 2011, Self-medication of migraine and tension-type headache: summary of the evidence-based recommendations of the Deutsche Migräne und Kopfschmerzgesellschaft (DMKG), the Deutsche Gesellschaft für Neurologie (DGN), the Österreichische Kopfschmerzgesellschaft (ÖKSG) and the Schweizerische Kopfwehgesellschaft (SKG) PubMed Central
- Dellermalm J et al, 2009, Caffeine does not attenuate experimentally induced ischemic pain in healthy subjects PubMed
- Henderson-Smart et al, 2010, Methylxanthine treatment for apnoea in preterm infants Cochrane
- 2007, Caffeine and health European Food Information Council
- Morillo LEE, Migraine headache in adults PubMed
- Riesenhuber A et al, 2006, Diuretic potential of energy drinks PubMed
- Neuhäuser-Berthold, 1997, Coffee consumption and total body water homeostasis as measured by fluid balance and bioelectrical impedance analysis PubMed
- Lohsiriwat S et al, 2011, Effect of caffeine on bladder function in patients with overactive bladder symptoms PubMed
- Interstitial cystitis MedlinePlus
- Kawachi I et al, 1994, Does coffee drinking increase the risk of coronary heart disease? Results from a meta-analysis PubMed Central
- van Dam RM et al, 2005, Coffee consumption and risk of type 2 diabetes: a systematic review PubMed
- Rosenberg L et al, 1988, Coffee drinking and nonfatal myocardial infarction in men under 55 years of age PubMed
- Cornelis MC et al, Coffee, CYP1A2 genotype, and risk of myocardial infarction PubMed
- Panagiotakos DB et al, 2003, The J-shaped effect of coffee consumption on the risk of developing acute coronary syndromes: the CARDIO2000 case-control study PubMed
- Mosqueda-Garcia M et al, 1990, Effects of caffeine on baroreflex activity in humans PubMed
- van Dam RM et al, 2006, Coffee, caffeine, and risk of type 2 diabetes: a prospective cohort study in younger and middle-aged U.S. women PubMed
- Cameron OG et al, 1990, Caffeine and human cerebral blood flow: a positron emission tomography study PubMed
- Pelligrino DA et al, Caffeine and the Control of Cerebral Hemodynamics PubMed Central
- Mathew RJ et al, 1985, Caffeine Induced Changes in Cerebral Circulation Stroke
- 2015, Usual Caffeine Consumption and Health Health.gov
- Santos C et al, 2010, Caffeine intake and dementia: systematic review and meta-analysis PubMed
- Hewlett P et al, 2006, Correlates of daily caffeine consumption PubMed
- Coffey RJ et al, 1986, The acute effects of coffee and caffeine on human interdigestive exocrine pancreatic secretion PubMed
- Cibicková E et al, 2004, The impairment of gastroduodenal mucosal barrier by coffee PubMed
- Stomach and Duodenal Ulcers (Peptic Ulcers) John Hopkins Medicine
- Anand BS, Peptic Ulcer Disease Emedicine
- Murao T et al, 2011, Lifestyle Change Influences on GERD in Japan: A Study of Participants in a Health Examination Program PubMed Central
- Zivković R, 2000, Coffee and health in the elderly PubMed
- Giacosa A et al, 1987, Dyspepsia among young conscripts: correlations with psychoemotional state and eating habits PubMed
- Akimoto K et al, 2009, Does postprandial coffee intake enhance gastric emptying?: a crossover study using continuous real time 13C breath test (BreathID system) PubMed
- Michels KB et al, Coffee, Tea, and Caffeine Consumption and Incidence of Colon and Rectal Cancer PubMed
- Matrana MR et al, Epidemiology and Pathophysiology of Diverticular Disease PubMed Central
- Ruhl CE et al, 2000, Association of coffee consumption with gallbladder disease PubMed
- Agardh EE et al, 2004, Coffee consumption, type 2 diabetes and impaired glucose tolerance in Swedish men and women PubMed
- Grenberg JA et al, 2005, Coffee, tea and diabetes: the role of weight loss and caffeine PubMed
- Campos-Outcalt D et al, 2012, Medical Marijuana for the Treatment of Migraine Headaches: An Evidence Review Arizona Department of Health Services
- MacKenzie T et al, 2007, Metabolic and hormonal effects of caffeine: randomized, double-blind, placebo-controlled crossover trial PubMed
- Kalra AA et al, 2007, Acute migraine: Current treatment and emerging therapies PubMed Central
- Robinson LE et al, 2004, Caffeine ingestion before an oral glucose tolerance test impairs blood glucose management in men with type 2 diabetes PubMed
- Vilarim MM et al, 2011, Caffeine challenge test and panic disorder: a systematic literature review PubMed
- Petrie HJ et al, 2004, Caffeine ingestion increases the insulin response to an oral-glucose-tolerance test in obese men before and after weight loss PubMed
- Ohnaka K et al, 2012, Effects of 16-Week Consumption of Caffeinated and Decaffeinated Instant Coffee on Glucose Metabolism in a Randomized Controlled Trial PubMed Central
- Katsarava Z et al, 2012, Defining the Differences Between Episodic Migraine and Chronic Migraine PubMed Central
- Elbers RG et al, 2015, Treatment for fatigue in Parkinson’s disease Cochrane
- van Dam RM et al, 2008, Coffee consumption and risk of type 2 diabetes, cardiovascular diseases, and cancer PubMed
- Arab L, 2010, Epidemiologic evidence on coffee and cancer PubMed
- Nkondjock A, 2009, Coffee consumption and the risk of cancer: an overview PubMed
- Brent RL et al, 2011, Evaluation of the Reproductive and Developmental Risks of Caffeine PubMed Central
- Momoi N et al, 2008, Modest maternal caffeine exposure affects developing embryonic cardiovascular function and growth PubMed
- Ephedra Drugs.com
- Liu H et al, 2012, Coffee consumption and risk of fractures: a meta-analysis PubMed Central
- Caffeine Content in Espresso vs Drip Coffee Coffeechemistry.com
Caffeine Effects, Half-Life, Overdose, Withdrawal
What is caffeine?
Caffeine is not a nutrient but a drug that is a mild stimulant of the central nervous system [2]. In regular caffeine consumers, a partial or complete tolerance to most of caffeine effects often develops [32,36,38,39].
Chemical and Physical Properties
Caffeine is an alkaloid–a natural, alkaline nitrogen-containing compound–with the chemical name 1,3,7-trimethylxanthine and chemical formula C8H10N4O2 [1].
Pure caffeine is an odorless, white, crystalline powder of bitter taste, soluble in water, fats and alcohol [1].
Production
Caffeine can be extracted from the coffee beans [5], tea leaves [6], kola nuts [7], cocoa pods [8], guarana seeds [9], yerba maté [9]. Caffeine can be also artificially synthesized [2].
Chat 1. Caffeine Sources |
|
| SOURCE | AMOUNT OF CAFFEINE in mg (range) |
| COFFEE | |
| Brewed, decaffeinated (8 oz, 237 mL) | 5 (2-12) |
| Espresso, restaurant style, decaffeinated (1 oz, 30 mL) | 5 (0-15) |
| Espresso, restaurant style (1 oz, 30 mL) | 40 (30-90) |
| Instant (8 oz, 237 mL) | 70 (30-170) |
| Drip coffee (8 oz, 237 mL) | 100 (65-120) |
| Brewed, Arabica (8 oz, 237 mL) | 100 (70-120) |
| Fast-food-size coffee (16 oz, 480 mL) | 125 (100-330) |
| Brewed, Robusta (8 oz, 237 mL) | 150 (130-220) |
| TEA | |
| Herbal and fruit tea | 0 |
| Black tea, decaffeinated (8 oz, 237 mL) | 5 (0-12) |
| Iced tea (8 oz, 237 mL) | 10 (5-50) |
| Kombucha tea (8 oz, 237 mL) | 25 |
| Green, black, white and oolong tea (8 oz, 237 mL) | 40 (15-110) |
| Other teas (8 oz, 237 mL) | Up to 70 (0-120) |
| SOFT DRINKS | |
| Cola, soda, root beer; caffeinated (12 oz, 355 mL) | 40 (30-120) |
| ENERGY DRINKS (4-10 oz, 120-300 mL) | 100 (50-280) |
| 1 can (4-16 oz, 120-480 mL); smaller cans do not necessarily contain less caffeine | 80 (30-350) |
| Caffeinated water (16.9 oz, 500 mL) | 50-100 |
| CAFFEINATED ALCOHOLIC BEVERAGES (CABs) | |
| 1 can (8-23.5 oz, 240-695 mL); smaller cans do not necessarily contain less caffeine | 100 (20-350) |
| OTHER BEVERAGES | |
| Coffee liqueur (1 jigger, 1.5 oz, 45 mL) | 4 |
| Caffeinated vodka (1 jigger, 1.5 oz, 45 mL) | 10 |
| Hot chocolate (6 oz, 180 mL) | 4 |
| Milk with cocoa (1 cup, 237 mL) | 5 |
| FOODS | |
| Chocolate cake (1 piece, 3.5 oz, 100 g) | 0-6 |
| Milk chocolate (1 oz, 28 g) | 6 |
| Dark chocolate, 70-85% cacao (1 oz, 28 g) | 23 |
| Ice creams and yogurts – caffeinated (8 oz, 237 mL) | 50 (8-85) |
| Mints with caffeine (1 mint) | 10-100 |
| Chewing gum – caffeinated (1 piece) | 50 (40-100) |
| Chocolate chips (1 cup) | 105 |
| Dark chocolate-coated coffee beans (28 pieces, 40 g) | 335 |
| MEDICATIONS and SUPPLEMENTS [34,35] | |
| Analgesics, diuretics, weight-loss pills, stimulants with caffeine (1 tablet or capsule) | Up to 400 |
| Workout supplements (1 serving) | Up to 400 |
Chart 1 sources: [10,11,12,13,14,15,16,223]
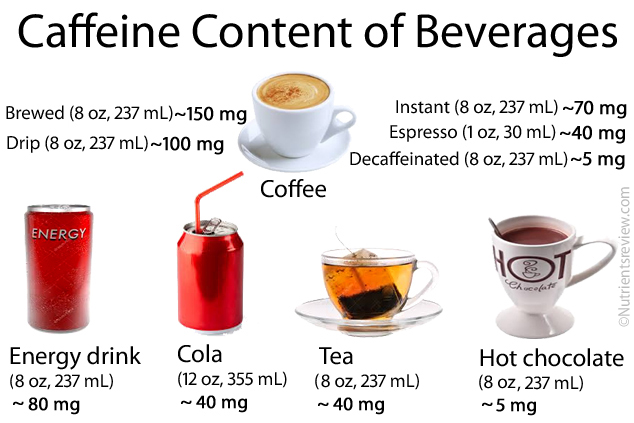
Picture 1. Caffeine content of common beverages
Caffeine Absorption, Distribution, Metabolism and Elimination
Absorption
99% of caffeine is absorbed in the stomach and small intestine within 45 minutes of ingestion [2,22,23]. Some caffeine from a chewing gum, chewable tablets and lozenges can be absorbed in mouth [29].
The caffeine dose, taking alcohol or oral contraceptives along with caffeine, exercise, age or sex do not significantly affect the caffeine absorption rate [2] but taking caffeine with food can slow it [29].
Caffeine Distribution and Blood Concentration
After absorption, caffeine is distributed throughout the body tissues, but it does not accumulate in them [2,29].
Caffeine may appear in the blood within 5 minutes [27] and reach its peak blood level within 15-120 minutes of consumption [25,27].
Ingestion of 1.1 mg of caffeine per kilogram of body weight may result in blood caffeine levels 0.5-1.5 mg/liter blood [25]. Drinking of 1 cup of coffee with different caffeine contents may result in blood caffeine levels ranging from 0.25 to 2 mg/liter [25].
Metabolism
Most of the consumed caffeine is broken down in the liver to theophylline, theobromine, paraxanthine and 1,3,7-trimethyluric acid with the help of the enzyme CYP1A2 [24,25]. Only about 1% of caffeine is excreted unchanged in the urine [2].
Elimination Half Life
The average elimination rate (clearance) of caffeine from the human body in adults is 155 mg/kg body weight/hour; in newborns it is ~30 mg/kg/h; it may reach adult levels at about 4th month of life [25,26].
The caffeine blood half life–the time in which 50% of caffeine is eliminated from the blood–in healthy non-smoking adults is about 3-8 hours [16,24,27]; in smokers it may be shorter by 30-50% [2,25] and in newborns may be longer than 80 hours [25].
Caffeine elimination half time may be prolonged when large amounts of caffeine are consumed (16 hours in one case) [28], in the last trimester of pregnancy (up to 15 hours), in women taking oral contraceptives (by ~50%), in regular alcohol drinkers (by ~70%) and in individuals with liver cirrhosis (up to 96 hours) [2,25].
Caffeine Effects and Mechanism of Action
Caffeine effects depend on the individual genetically determined caffeine sensitivity [50] and tolerance [51], caffeine dose, expectancy of the effects [55,56,57] and eventual drugs consumed along with it [22,24]. Caffeine effects (400 mg or 2 cups of coffee) may appear within less than 1 hour and last for 3-6 hours or more [47].
Caffeine inhibits the inhibitory effects of the neurotransmitter adenosine and thus acts as a mild stimulant of the central nervous system [22,30].
Acute caffeine consumption stimulates the release of norepinephrine (noradrenaline) and epinephrine (adrenaline) in the body, which results in increased breakdown of the body fats into fatty acids [33,40], increased synthesis of glucose (gluconeogenesis), breakdown of glycogen into glucose (glycogenolysis) and dilation of bronchi [27,31,33]. Caffeine in a dose 6 mg/kg body weight (2-3 cups of coffee) can increase epinephrine release during exercise by about 40% [33].
In some studies, caffeine increased the basal or resting metabolic rate [41,42,43,44], but it did not in others [45].
According to some studies, caffeine may have a thermogenic effect [40,41,52,53,54], but according to others it does not [45]. Results of studies about caffeine effect on the body temperature are inconclusive [47].
In regular caffeine consumers a partial or complete tolerance to the abovementioned caffeine effects often develops [32,36,38,39].
Moderate and Excessive Caffeine Intake
Consumption of up to 200-300 mg of caffeine (~2 cups of coffee) per day is considered moderate intake and of more than 500-600 mg (> 5 cups of coffee) per day heavy or excessive intake [48,49].
Possible Caffeine Benefits
- Increased alertness and vigilance, probably more in tired in sleepy individuals than those who are already alert [58,59,60,61,62,134,135].
- Shorter reaction time [64,65,67]
- Improved athletic performance during endurance exercise lasting more than 30 minutes (running) [28,45,68,103,138,139,140]
- A slight increase of the analgesic effect of aspirin, acetaminophen and ibuprofen [72,73,74,75], for example in tension headache [172].
NOTE: Improved mood and performance often reported by regular caffeine consumers may be due to reversal of withdrawal symptoms by consuming caffeine rather than by the effect of caffeine itself [66]. In regular caffeine consumers a partial or complete tolerance to most of caffeine effects often develops [32,36,38,39].
There is INSUFFICIENT EVIDENCE about the beneficial effects of caffeine consumption athletic performance during short-term exercise, such as sprints or lifting [115], attention deficit hyperactivity disorder (ADHD) [89], asthma [85,86], cognitive function in Alzheimer’s disease [191,192], depression [115], diabetes mellitus type 2 [22,23,187,205], gallstones [87,88], gout [83,84], hepatitis C or liver cirrhosis [115], improving breathing in preterm infants with apnea [150,174], leg cramps due to narrowed arteries (intermittent claudication) [115], liver cancer [191], memory [16,67], migraine headache [176,207,209] ,muscle soreness during exercise [115], obsessive-compulsive disorder (OCD) [115], orthostatic hypotension [78,80], postprandial hypotension (a drop of blood pressure after meals) [77], seizures [25], skin itching [115], stroke [115] or weight loss [90].
Caffeine and Sleep
Caffeine may help overcome sleepiness after awakening (sleep inertia), possibly by increasing blood cortisol levels [37,38,160].
Caffeine, generally in amounts greater than 200 mg (~1-2 cups of coffee), consumed up to 8 hours before bed, may delay the sleep onset, shorten the sleeping time and decrease the sleep quality, more likely in occasional than regular users [16,25].
Caffeine, Brain, Memory and Behavior
The consumption of 250 mg of caffeine (1-2 cups of coffee) in a single dose can constrict the brain arteries and decrease the brain blood flow by up to 30% [188,189]. It is not yet clear if this increases the risk of stroke or transient ischemic attack [189,190].
Caffeine consumption probably does not have any significant effect on memory while studying [16,67]. A good sleep or daytime nap can have better effect on the learning performance than consuming caffeine [161].
In one 2006 study, there was no association between caffeine consumption and impulsiveness, sociability, extraversion or trait anxiety [130,193].
Caffeine and Exercise Performance
In 2004, caffeine was removed from the World Anti-Doping Agency (WADA) list of prohibited substances [137].
Caffeine in doses 3-9 mg/kg of body weight may modestly increase the endurance performance and decrease fatigue during physical exercise lasting for more than 30 minutes [28,45,68,103,138,139,140]. In some studies, caffeine consumption in doses 1-9 mg/kg body weight (1-7 cups of coffee) 60 minutes before exercise was associated with better short-term (<90 seconds) anaerobic physical performance, such as sprints or weight lifting [145,146,147,148,149] but in others was not [103,142,143,144].
It is not clear which caffeine dose has the optimal effect on physical performance; repeated bouts of coffee may decrease it [45,68,138].
Caffeine in high doses (8 mg/kg body weight or ~5 cups of coffee) may help restore glycogen stores after exercise [151].
At doses higher than 3 mg/kg, caffeine may increase heart rate during exercise [152].
Caffeine does not likely cause hyperthermia or heat intolerance during exercise in a hot environment [91,93].
Caffeine added to sport drinks does not seem to increase the risk of gastrointestinal symptoms during exercise [153].
It is still not clear by which mechanism caffeine could increase physical performance. Possible mechanisms: increasing caffeine doses are associated with increased blood epinephrine levels [154,155,156], calcium availability in the cells [16] and glucose absorption [157].
Caffeine, Appetite and Weight Loss
In some studies [25,163,164], caffeine consumption was associated with lower appetite, but in others it was not [37,54,162].
In several short-term studies taking caffeine-ephedrine supplements, but neither ephedrine or caffeine alone, was associated with weight loss of 1-2 pounds per month, but the long-term effect of caffeine on weight loss is not known [165,166,167,168]. These supplements are not approved as weight-loss pills in the U.S., since they may have serious side effects, including death [167].
In some studies [41,163], caffeine alone in doses 150-300 mg/day was associated with weight loss, but in others it was not [90].
There is insufficient evidence about the effectiveness of black or green tea in promoting weight loss [169,170].
Caffeine, Frequent Urination and Dehydration
In several studies, consumption of up to 226 mg of caffeine (~2 cups of coffee) did not result in any significant increase in urine excretion (diuresis) [69,91]. Acute ingestion of at least 240 mg of caffeine (1-2 cups of coffee or 5-6 cups of tea) may temporarily increase the urine excretion, but the tolerance to this caffeine effect may develop in as little as 1 day [92,177]. In conclusion, caffeinated beverages consumed by healthy individuals in usual doses do not likely cause dehydration and can be even used for rehydration [28,69,91,92,141].
In individuals with overactive bladder or urge incontinence [179], or a non-infectious bladder inflammation called interstitial cystitis or painful bladder syndrome (PBS), caffeine consumption may trigger urination urgency and increase urination frequency [179,180].
Coffee, Caffeine and Heart
In some studies, moderate coffee drinking (3-5 cups/day) was associated with a lower risk of cardiovascular disease [49,70,76, 185], but in others it was not [22,181]. It is not clear is it caffeine or some other substance in coffee that might be associated with a lower risk of heart disease.
Regular caffeine consumption may increase the risk of heart attack in genetically predisposed individuals who metabolize (break down) caffeine slowly [183,184].
Caffeine and Blood Pressure
In non-regular caffeine consumers with or without hypertension, 250 mg of caffeine (2-3 cups of coffee) can temporarily (for several hours) increase the blood pressure by up to 15 mm Hg within 1 hour of consumption [63,116,186]. After few days of caffeine consumption, a partial or complete tolerance to caffeine-induced increase of the blood pressure usually develops, especially in those who consume more than 3 cups of coffee per day [25,117,126,186,191].
In individuals with hypertension, long-term coffee consumption does not seem to be associated with an increase of blood pressure [63,136].
Currently, it is not clear, if regular caffeine consumption increases the blood pressure to the harmful levels. If you have high blood pressure, ask your doctor how much caffeine you may consume.
Caffeine and Diabetes 2
In various systematic reviews of epidemiological studies, regular caffeine or coffee consumption was associated with a lower risk of diabetes type 2 [70,159,182,191] but, according to one study, only in individuals who had previously lost weight [206]. Possible preventative mechanisms of drinking coffee on diabetes include an increase of insulin sensitivity by caffeine and inhibition of glucose absorption by chlorogenic acid (a coffee ingredient) [23].
In various controlled clinical trials, decreased insulin sensitivity was observed after co-ingestion of carbohydrate meals and caffeine (200-500 mg, comparable with 1-5 cups of coffee) in healthy individuals [105,208] and in those with diabetes type 2 [158,210]. Possible mechanism: caffeine stimulates the release of epinephrine, which decreases the sensitivity of insulin.
In conclusion, the current evidence is not strong enough to recommend consuming caffeine as a preventative measure for diabetes.
Coffee and Gastrointestinal Tract
Coffee stimulates the release of the hormone gastrin and gastric acid secretion [101,194]. Caffeine may damage the gastric and duodenal lining [195] but does not likely cause peptic ulcer; it can increase pain in an established ulcer, though [77,196,197].
Caffeine, coffee and tea may decrease the pressure in the lower esophageal sphincter and trigger acid reflux and heartburn [101,102,198]. Decaffeinated coffee can also trigger heartburn [199].
In several studies there was no association between moderate coffee or tea consumption, dyspepsia and gastric emptying or bowel transit time [101,153,200]. However, according to one 2009 study, caffeine may accelerate gastric emptying [201]. Caffeine may promote the motility of the sigmoid colon and rectum [202].
In individuals with irritable bowel syndrome, caffeine may trigger diarrhea or constipation [101].
Caffeine intake does not seem to be associated with diverticular disease [203].
Coffee intake may induce gallbladder contractions and may cause pain in individuals with established gallstones [101], but it does not seem to increase the risk of gallstones or other gallbladder disease in healthy individuals [87,204].
Caffeine and Parkinson’s Disease
In some epidemiological studies, moderate coffee consumption was associated with a decreased risk of Parkinson’s disease in men [22,78,191]. There is lack of evidence about the effect of caffeine in improving fatigue in individuals with Parkinson’s disease [215].
Caffeine and Cancer
Several studies suggest that regular caffeine consumption may reduce the risk of liver [22,191,216,217] and endometrial cancer [191,217].
Some, but not all, studies suggest that coffee or caffeine may have a protective effect on kidney [218] and colorectal cancer [22].
Caffeine consumption does not seem to increase or decrease the risk of breast, pancreatic, ovarian or gastric cancer [217].
Caffeine consumption may increase the risk of bladder cancer in men [217].
Caffeine as an Analgesic
Caffeine may stimulate the release of beta-endorphins, which are endogenous opioids [103]. It is not clear if caffeine alone has any significant analgesic effect [25,171].
Caffeine in doses 100 mg or higher may slightly increase the perceived analgesic effect of certain painkillers, such as aspirin, paracetamol and ibuprofen [74], in treating headache, post-operative dental pain or pain after birth [72,73,75].
Caffeine does not seem to relieve ischemic pain (angina pectoris) in coronary artery disease [173].
There is insufficient evidence about the effectiveness of caffeine in relieving migraine headache [176,207,209,214].
Caffeine Safety
Caffeine is LIKELY SAFE for most adults when consumed in usual amounts found in beverages and foods [115].
Caffeine is POSSIBLY SAFE for most children when used in amounts usually found in beverages or foods (up to 160 mg per day in a 10 year old child) [115,175].
Caffeine as a food additive is considered Generally Recognized As Safe (GRAS) by the U.S. Food and Drug Administration (FDA) until used in cola-type beverages [3,4] and in alcoholic beverages [113] in amounts up to 0.02 percent (200 ppm) but not automatically when used in other foods.
In general, moderate caffeine intake (3-5 cups of coffee or up to 400 mg caffeine per day) does not seem to increase the risk of cardiovascular disease (heart attack or irregular heart rhythm) and cancer [191].
It is currently not clear if caffeine consumption increases the risk of osteoporosis and bone (hip) fractures [22,24,123,133,222].
Pregnancy
Caffeine is POSSIBLY SAFE during pregnancy when used in doses up to 200 mg/day (1-2 cups of coffee) [21,22,115].
Drinking caffeinated beverages during pregnancy, even in high amounts, does not seem to increase the risk of miscarriage, birth defects or growth retardation of the fetuses or children [2,96,191,219] but more studies are warranted [220].
Caffeine withdrawal symptoms, such as irritability and vomiting, lasting for few days after birth, have been observed in infants whose mothers had been drinking coffee during pregnancy [25].
Breastfeeding
Caffeine is excreted in the breast milk in small amounts [20]. Consumption of 2-3 cups of coffee probably does not cause adverse effects, but higher caffeine intake may cause irritability and poor sleeping in a breastfed child [20,22].
Acute Side Effects
Caffeine consumption may cause [89,97]:
- Anxiety, panic attack, depression, restlessness, sleeplessness [89,211] and worsening of premenstrual syndrome (PMS) [98,99]
- Dry mouth, unusual thirst [100]
- Increased breathing and heart rate, pounding heart (palpitations) [71,100]
- Stomach upset, heartburn, nausea, vomiting, diarrhea [96,100,101,102]
Caffeine Intoxication or Overdose
Consuming caffeine in a single dose as low as 250 mg, but usually in doses greater than 600 mg, may result in caffeine intoxication [28]. On the other hand, consumption of up to 900 mg (0.9 g) caffeine through the day without any side effects has been reported [2].
Symptoms and signs of caffeine intoxication may include [2,25,28,51,97,106,107,108]:
- Headache
- Nervousness, anxiety, jitters, restlessness, fear, insomnia, rambling flow of thoughts or speech
- Facial flushing
- Ringing in the ears (tinnitus), increased sensitivity to light (photophobia)
- Thirst, stomach upset, abdominal pain, nausea, vomiting, diarrhea
- Increased breathing (hyperventilation) and heart rate (tachycardia), irregular heart beat (arrhythmia), chest pain, high or low blood pressure
- Fever
- Increased urination (polyuria)
- Dilated pupils
- Seizures
- Tremor, muscle twitching, paralysis or weakness due to hypokalemia
- Depression, delirium, hallucinations, psychosis
- Complications may include heart attack, stroke, muscle disintegration (rhabdomyolysis), acute lung damage, collapse or coma
- References: [2,25,28,51,97,106,107,108]
Possible metabolic changes in caffeine intoxication include hyperglycemia, ketosis, lactic acidosis or hyponatremia [28]. Very high caffeine doses, for example, from caffeine-containing pills [28], 10 cups of coffee per day [109], 5 or more liters of caffeinated cola per day [110,111,112] may cause hypokalemia.
Death from caffeine toxicity is rare and can occur when blood caffeine concentration exceeds about 100 mg/liter [113]. Lethal dose of caffeine–the amount that would likely kill an adult–is 10-20 grams or 150-200 mg/kg body weight (~70-120 70 cups of coffee) [27,29,108,114].
Chronic Side Effects
Regular consumption of high amounts of caffeine may cause or worsen:
- Anxiety, restlessness, insomnia, tingling in limbs and around the mouth, pounding heart (palpitations), anorexia, nausea, vomiting, diarrhea, depression or seizures – a cluster of symptoms known as chronic caffeine intoxication or caffeinism, from > 1,000 mg caffeine (>cups of coffee) per day or, in some individuals, from as low as 250 mg caffeine (or 1-2 cups of coffee) per day [25,60,105].
- Frequent urination and other symptoms of benign prostate hyperplasia [79]
- Fibrocystic breast disease [105,122]
- Migraine [214]
- Psychosis in healthy individuals and in individuals with schizophrenia [121]
- Restless leg syndrome [119,120]
- Seizures in individuals with epilepsy [82,118]
Who should avoid caffeine?
Doctors may advise against consuming caffeine to [25,115]:
- Children under 12 years of age
- Individuals allergic to caffeine
- Individuals suffering from anxiety, attention deficit hyperactivity disorder (ADHD), benign prostatic hyperplasia, bipolar disorder, chronic headache, glaucoma, GLUT-1 deficiency, heart attack (within 1 week thereafter), insomnia, high blood pressure, interstitial cystitis, irregular heart rhythm, irritable bowel syndrome (IBS), liver problems, osteoporosis, premenstrual syndrome (PMS), seizures (epilepsy), stomach ulcers or urinary incontinence
In healthy persons, moderate caffeine intake (<400 mg/day) does not likely cause or increase the risk of cancer [2], dehydration [91,92], DNA errors (mutations) [2], electrolyte imbalance [91], elevated blood cholesterol [22], excessive sweating [103], heart disorders [22], high blood pressure [117], increased body temperature [93], inflammation [37] or stroke [94].
Caffeine Tolerance
Caffeine consumption for 1-5 days may result in a partial or complete tolerance to some caffeine effects and side effects [25,32,51,124,125]. The susceptibility to develop caffeine tolerance may vary greatly among individuals and may be genetically determined [51].
The tolerance for the following caffeine effects often occurs: anxiety, increase of blood pressure [126], increased heart rate and increased urination [16]. Less often, the tolerance for caffeine-induced alertness and sleep disturbances develops [16].
Caffeine tolerance can wear off in 20 hours to 4 days after caffeine consumption cessation [32,127].
Chronic caffeine consumers, because of the developed tolerance, may have no net benefits from caffeine, and that increased alertness and performance they experience are in fact a reversal of withdrawal symptoms (“withdrawal relief”) [65,66,128,129].
Caffeine Addiction
A long-term caffeine consumer who experiences withdrawal symptoms, such as headache and tiredness, after abruptly stopping consuming caffeine is considered physically addicted to caffeine [25]. People who are physically addicted to caffeine usually do not have any significant social or health problems related to caffeine [25].
Caffeine Withdrawal
Some individuals who regularly consume caffeine for as little as 3 days in the row in doses as low as 100 mg (1/2 cup of coffee) develop symptoms of caffeine withdrawal 3-36 hours after the last dose of caffeine [16,25,51,130,131,132]. Symptoms usually peak between 20-51 hours after the last caffeine dose, last from 2-9 days and may include [16,25,51,132]:
- Headache
- Apathy, depression, tiredness, weakness, fatigue, drowsiness or insomnia
- Anxiety or irritability, difficulty concentrating
- Increased heart rate
- Nausea, vomiting or flu-like symptoms, such as stuffy nose
- Muscle aches or stiffness
Gradual caffeine withdrawal may result in fewer unpleasant symptoms than abrupt withdrawal [130].
Caffeine withdrawal headache is hardly relieved by usual analgesics, but may be relieved by caffeine within 30 minutes of the headache onset [25].
Caffeine Hypersensitivity
Some people can experience jitteriness, sleeplessness and irritation of gastrointestinal tract after small amounts of caffeine, for example, after drinking 1 cup of coffee [50]. Hypersensitivity results from low amount of enzymes that break down caffeine, which can be genetically determined [50].
Caffeine Allergy and Intolerance
In sensitive persons, caffeine ingestion may trigger allergic reaction with rash, hives, itching, difficulty breathing, tightness in the chest, or swelling of the face, lips and tongue [105].
Caffeine intolerance as a medical term is not known, but individuals with irritable bowel syndrome (IBS) may experience worsening of symptoms (constipation or diarrhea) after caffeine consumption [101].
Caffeine-Drug and -Nutrients Interactions
Caffeine-Nutrients Interactions
- Caffeine may slightly decrease calcium absorption [19,22].
- Caffeine added to sport drinks enhances the absorption of glucose in the small intestine [153].
Caffeine-Alcohol Interactions
- Caffeine does not affect the rate of alcohol absorption or elimination and does not affect the blood alcohol concentration [2].
- Caffeine may decrease the feeling of sedation after alcohol intoxication, but it does not reduce the intoxication itself [17,18].
- Alcohol does not affect caffeine absorption, but it slows down its elimination; caffeine from alcoholic beverages does not likely cause unsafe blood caffeine levels, though [2].
Other Caffeine-Drug Interactions
- Caffeine in combination with ephedrine can have serious side effects including death [115,221].
- Caffeine may increase the effects and side effects of acetaminophen, albuterol, aspirin, clozapine, epinephrine and theophylline [22].
- Caffeine may decrease the effects of lithium [24] and diazepam [178].
- Drugs that may increase caffeine effects include certain antibiotics (erythromycin, ciprofloxacin, norfloxacin) cimetidine, disulfiram, echinacea (herbal supplement) erythromycin, mexiletine, oral contraceptives [22,24,27].
- Smoking (nicotine) can decrease caffeine levels by stimulating caffeine elimination by 30-50% [25].
Alcohol
- Alcohol chemical and physical properties
- Alcoholic beverages types (beer, wine, spirits)
- Denatured alcohol
- Alcohol absorption, metabolism, elimination
- Alcohol and body temperature
- Alcohol and the skin
- Alcohol, appetite and digestion
- Neurological effects of alcohol
- Alcohol, hormones and neurotransmitters
- Alcohol and pain
- Alcohol, blood pressure, heart disease and stroke
- Women, pregnancy, children and alcohol
- Alcohol tolerance
- Alcohol, blood glucose and diabetes
- Alcohol intolerance, allergy and headache
- Alcohol and psychological disorders
- Alcohol and vitamin, mineral and protein deficiency
- Alcohol-drug interactions
- Fructose
- Galactose
- Glucose
- Isomaltose
- Isomaltulose
- Lactose
- Maltose
- Mannose
- Sucrose
- Tagatose
- Trehalose
- Trehalulose
- Xylose
- Erythritol
- Glycerol
- Hydrogenated starch hydrolysates (HSH)
- Inositol
- Isomalt
- Lactitol
- Maltitol
- Mannitol
- Sorbitol
- Xylitol
- Fructo-oligosaccharides (FOS)
- Galacto-oligosaccharides (GOS)
- Human milk oligosaccharides (HMO)
- Isomalto-oligosaccharides (IMO)
- Maltotriose
- Mannan oligosaccharides (MOS)
- Raffinose, stachyose, verbascose
- SOLUBLE FIBER:
- Acacia (arabic) gum
- Agar-agar
- Algin-alginate
- Arabynoxylan
- Beta-glucan
- Beta mannan
- Carageenan gum
- Carob or locust bean gum
- Fenugreek gum
- Galactomannans
- Gellan gum
- Glucomannan or konjac gum
- Guar gum
- Hemicellulose
- Inulin
- Karaya gum
- Pectin
- Polydextrose
- Psyllium husk mucilage
- Resistant starches
- Tara gum
- Tragacanth gum
- Xanthan gum
- INSOLUBLE FIBER:
- Cellulose
- Chitin and chitosan
- FATTY ACIDS
- Saturated
- Monounsaturated
- Polyunsaturated
- Short-chain fatty acids (SCFAs)
- Medium-chain fatty acids (MCFAs)
- Long-chain fatty acids (LCFAs)
- Very long-chain fatty acids (VLCFAs)
- Monoglycerides
- Diglycerides
- Triglycerides
- Vitamin A - Retinol and retinal
- Vitamin B1 - Thiamine
- Vitamin B2 - Riboflavin
- Vitamin B3 - Niacin
- Vitamin B5 - Pantothenic acid
- Vitamin B6 - Pyridoxine
- Vitamin B7 - Biotin
- Vitamin B9 - Folic acid
- Vitamin B12 - Cobalamin
- Choline
- Vitamin C - Ascorbic acid
- Vitamin D - Ergocalciferol and cholecalciferol
- Vitamin E - Tocopherol
- Vitamin K - Phylloquinone
- Curcumin
- FLAVONOIDS:
- Anthocyanidins
- Flavanols: Proanthocyanidins
- Flavanones: Hesperidin
- Flavonols: Quercetin
- Flavones: Diosmin, Luteolin
- Isoflavones: daidzein, genistein
- Caffeic acid
- Chlorogenic acid
- Lignans
- Resveratrol
- Tannins
- Tannic acid
2 Responses to "Caffeine Effects, Half-Life, Overdose, Withdrawal"